
A Fragile State of Health: COVID-19 in Africa
Executive Summary
- The novel coronavirus disease (COVID-19) pandemic is putting particular strain on Africa’s fragile states, which are struggling to deal with long-standing threats while trying to rally mistrustful and recalcitrant publics, all without a clear idea of COVID-19’s progression in the population.
- Domestically, African governments should find ways to communicate to their citizens knowledge, concern, and resolve in fighting COVID-19, while developing pragmatic “social distancing” approaches in collaboration with civil society and ordinary citizens.
- Internationally, stronger African countries should come together as they emerge from national coronavirus emergencies in order to help lift the continent into recovery, while the African Union assumes its role as advocate on the global stage for the region’s interests in the post-coronavirus world order.
A novel strain of very contagious respiratory coronavirus is spreading rapidly around the globe, changing the rhythms of human life in fundamental ways. In Africa, the pandemic’s trajectory and the continent’s vulnerabilities are aligning to put considerable pressure on fragile states. Extremely weak states—South Sudan, Somalia, Central African Republic, and the Democratic Republic of the Congo (DRC)—find themselves largely exposed before the virus; high performers—Botswana, Tunisia, Senegal, and the Seychelles—are managing to pull through for now. But most African states are somewhere in between. Thirty-two of Africa’s fifty-four countries lie in the deciles on either side of the “Warning” and “Alert” categories in the 2019 Fragile State Index (FSI). Each has its own particular COVID-19 risk profile, but taken together, these countries present a continent in peril. How harmful the health crisis will be remains an open question. The coronavirus pandemic challenges African states in terms of legibility,1 authority, and capacity. Actions taken now, especially in the thirty-two borderline fragile states, could affect security and governance in Africa and beyond for years to come.
Entering a Blind Curve
COVID-19 is working its way—person by person, place by place—into social spaces large and small, in Africa and around the world. To craft finely-tuned interventions that curb the pandemic, government officials must be able to “see like a state”; they need the tools that make the nation “legible,” that is, the detailed data, mappings, and metrics of the individuals, resources, and conditions in their territory that would allow for precise management and tailored guidance of the population.2 Yet African policy-makers sitting in offices in the capital cities of borderline fragile states rarely have those tools of statecraft at their disposal.
Africa faces several obstacles to flattening the curve. Measures meant to stave off COVID-19 infections—known as “social distancing”—simply cannot be applied in numerous cramped and neglected pockets of poverty on the continent. Staying at home is not an option for the millions who set out each morning hoping to earn their daily bread. Self-isolating is not possible for extended families sharing a single room where everyone eats, sleeps, and lives. Washing hands regularly cannot be done in places without running water.3
Africa is also poorly positioned to benefit from a potentially flattened curve. There is limited capability to ramp up production of masks, respirators, or intensive care unit beds, or to import them from countries in the throes of their own coronavirus crises. And African healthcare systems are so frail, even drastically reduced caseloads will overwhelm them. Equipment and training is sorely lacking. Congo has just ten respirators in the country; Niger has five, Togo has four.4 Doctors and nurses have gone on strike in Zimbabwe because they lack the training and protective gear necessary for dealing with COVID-19 cases.5 FSI figures show the breadth of Africa’s healthcare vulnerability. Indicators for “public services” and “demographic pressures”—which measure inter alia things like number of clinics, hospitals, and medical professionals; access to medicine, potable water, and adequate sanitation systems; ability to control disease; and presence of epidemics—actually raise the fragility score in sub-Saharan Africa by an average of roughly six percent.6 In other words, measures for provision of services like healthcare generally exacerbate—rather than mitigate—African state fragility.
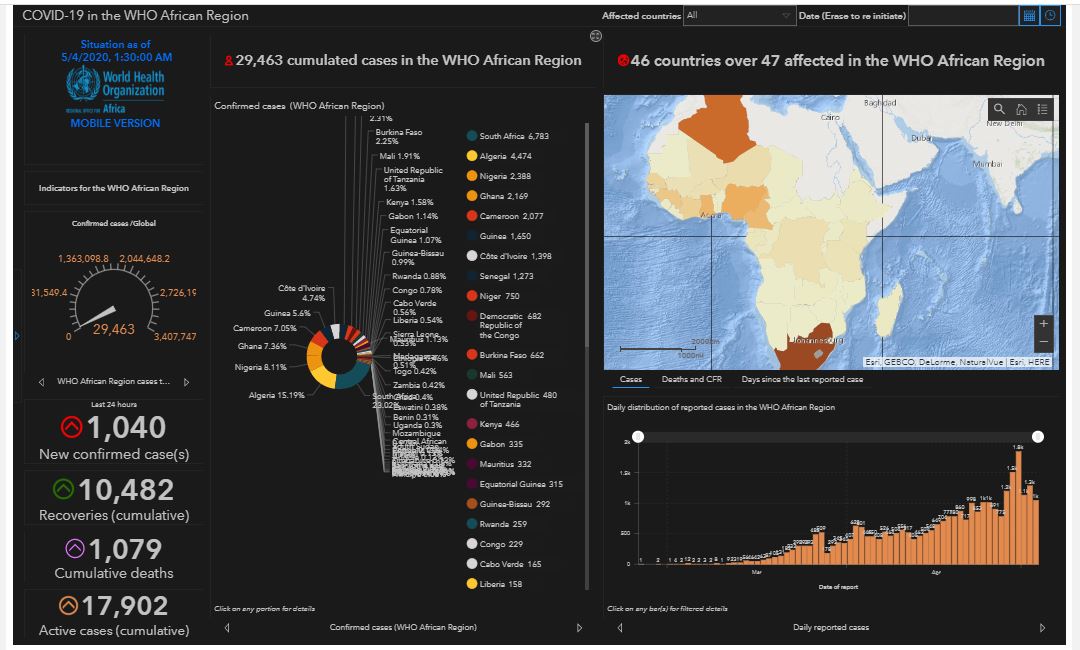
Statistics of COVID-19 cases coming from the continent are doubtful; the numbers must be higher than reported. At the end of March, Ethiopia, a country of 108 million people, counted twenty-five confirmed cases, about three-quarters of the number (thirty-four cases) posted by the island nation of Barbados, population 300,000. Africa’s most populous nation, Nigeria, reported that its 214 million inhabitants had a total of 135 cases, roughly on par with Brunei, whose 460,000 inhabitants registered 129 cases. 7 Such figures indicate infection rates around twenty-five times lower than Singapore, sixty times lower than South Korea, and 1,000 to 2,000 times lower than the United States. It is hard to imagine these statistics actually reflect how the coronavirus is operating, for example, in megacities like Lagos, the world’s fourth most densely populated city8 in the country with the largest number of people living in extreme poverty.9 Massive case rates may not mean mass casualties in Africa, since COVID-19 mortality rates are highest for people in their seventies and eighties and life expectancy in Africa is the lowest of all continents, at sixty-five for women and sixty-one for men.10 Yet with cases rising, the crisis is real. Worried about COVID-19’s rapid but silent spread across the continent, a scientist in South Africa has called the coronavirus in Africa a ticking time bomb.11
Unable to grasp with precision the actual situation, African officials seem nonetheless determined to impose their numbers and narrative by force. A Nigerien blogger was arrested for “disturbing public order” for reporting on a suspected coronavirus case in Niamey, while a British journalist was forced out of Egypt for publishing a story questioning the country’s official coronavirus statistics.12 In nearly a dozen countries across Africa, COVID-19 coverage has been linked to new forms of press intimidation and limitations, fines and legal sanctions, and abuse of journalists by authorities.13 The actual magnitude and implications of COVID-19 on the continent will not become apparent for weeks or months to come and the total effect may never be fully measured.

Social Cont(r)act
COVID-19 is at once an intangible and tangible threat. On the one hand, the disease can be rather mild for many who catch it. Coronavirus symptoms often mimic a common cold; some sick people experience no symptoms at all. Infection passes undetectably from one person to another, taking a week or two to show signs of illness. The vast majority—four out of five with coronavirus—recover with no special medical treatment. On the other hand, for the final fifth, COVID-19 is very serious. It damages the immune system and lungs in ways that require intensive medical attention and can cause death,14 with the victims’ last days spent out of sight, where they live or in a hospital ward.
Responses, by contrast, invert the concrete and abstract elements of the disease. Everyone sacrifices to save the most vulnerable citizens; everyday acts of “social distancing” are done for a suffering minority that remains largely at a remove from the public at large. Combatting a disease with COVID-19’s profile, therefore, requires social solidarity and a unity of purpose in pursuing the common good. It requires social trust in legitimate leaders who speak with a credible voice and convey clear decisions. It also requires effective institutions, those “humanly devised formal and informal rules and constraints that structure political, economic, and social interaction so as to create order and reduce uncertainty.”15
But this very connection—the bond between nation and state—is frail or deficient in Africa’s borderline fragile “nation-states.” These governments do not have strong institutions and state capability: they often struggle to achieve a baseline monopoly on the legitimate use of force in their territory. They do not enjoy a robust sense of trust and solidarity throughout society; privileged sectors purchase even security for themselves through high walls, metal gates, and personal guards. In such places, cabinet ministers are unlikely to inspire confidence when speaking to the country about case numbers or testing results. Heads of state can hardly expect to generate a genuine esprit de corps around “social distancing” protocols among inhabitants who feel disregarded by what they consider a corrupt system that was never build for their welfare. Politicians and officials in these places lack the authority necessary to unite and lead the nation in the fight against the virus.
If anything, the coronavirus seems to be reducing popular participation and distancing the political system from the people in most of Africa. COVID-19 restrictions have put an end to mass opposition demonstrations in Zimbabwe and in Algeria,16 where they had continued every week for over a year. Tanzania’s prime minister has banned all political rallies. Burundi plans to hold elections in May, but Côte d’Ivoire and Ethiopia have delayed elections scheduled later this year.17 Suspicion that politicians plan to use the coronavirus for a power grab is widespread. When Guinea-Bissau followed Mozambique and declared a state of emergency, critics claimed the government did so simply to suppress debate.18
Instead, many ordinary Africans, living through a time of distress, are turning to their communities—determined by locality, ethnicity, religion (in other words, identities other than nationality)—in order to ensure their immediate physical security and basic economic needs. These community connections make for resilience among African people, and these bonds are built disproportionately on social contact—in the market, in the street, or (in arguably the most religious continent on Earth)19 in the church or mosque. Unsurprisingly, vulnerable and anxious individuals who rely on direct, personal networks to survive may desire to reaffirm, rather than forego, face-to-face interactions at this time.

Thus, the COVID-19 dynamic is shaping up to pit social contract against social contact, government against community, the state against its own citizens. The tension appears in divisions between political and religious guidance.20 Many Nigerians insist on going to church despite warnings by the government.21 In Cameroon, Muslims denounced mosque closings as defying God’s teachings and assembled in spite of government restrictions.22 African officials have been relatively circumspect in their demands. Nigeria aims to keep social gatherings to groups of fifty23; Malawi and Zimbabwe have limited public gatherings to 100.24 Yet even this level of distancing has proven difficult to enforce. Dozens of Kenyans across several cities have been injured in the application of COVID-19 regulations25 and demonstrators protesting in the face of government bans in Niger have suffered a dozen arrested and three deaths. Struggling to enforce decisions, governments have turned to their militaries. In Fez, Tangiers, and Tétouan, Moroccans defying orders to pray at home have precipitated government deployment of military patrols.26
The fight between the state and the people is playing out primarily in densely populated poor or working-class urban neighborhoods.27 “We don’t want it!,” inhabitants of Yopougon, a commune of five million in Abidjan, Côte d’Ivoire, recently shouted as they violently dismantled a temporary shelter set up to treat coronavirus, fearing a concentration of the infected in their neighborhood.28 Soldiers fired rubber bullets at hundreds of South Africans who came out to shop in groups in the neighborhood of Yoeville in Johannesburg.29 Kenyan police are patrolling Nairobi neighborhoods like Kibera, the so-called largest slum in Africa,30 beating with batons citizens who disobey a dusk-to-dawn curfew. By April 2, police violence against violators had taken the lives of five Kenyans, more than the virus itself.31
In time, the battle may extend to secondary and tertiary urban centers, where regional specificity and center-periphery dynamics could come into play; eventually violence over enforcement of “social distancing” measures could move to the borderlands and the bush. At present, African regimes are trying to get their people to obey the restrictions through carrot and stick, especially the latter in areas where the state has never really held full sway. This dynamic of coercion and violence will have long-term implications for governance and security in Africa.
No Relief
COVID-19 is itself a hard problem and it makes other problems harder. The pandemic is a health crisis that is also an opportunity for criminal profiteering and corruption. At the same time, COVID-19 saps resources needed to confront traditional threats, placing a strain on the capacity of fragile states to provide security under adversity.
Refugee camps in African countries, for example, face particularly tough circumstances. Africa has twenty-five million displaced persons, many of them living by the tens or hundreds of thousands in official or makeshift camps. The coronavirus crisis makes improving their health and sanitation services all the more urgent; it also requires making it safe for illegal migrants to “come out of the shadows” when sick. So far governments have focused on trying to isolate the camps. Uganda, host to 1.2 million refugees, has suspended all new refugee arrivals for a month; Borno state, where thirty-two official camps house most of Nigeria’s 2.6 million internally-displaced persons, has banned all visitors.32
Meanwhile, African states are taking the opposite tack with prisons, which they fear could become centers of contagion that spin out of control. Human rights organizations assess high vulnerability to COVID-19 given the jail conditions in places like Madagascar33 and prisoners have rioted against visitor restrictions in Chad, leading to five deaths and thirty escapees.34 To alleviate the tension, several countries have decided to simply let the imprisoned go. Morocco has released more than 5,600 prisoners35 and Niger’s president pardoned 1,540 convicts in order to reduce the incarcerated population.36 Political activists and opposition figures are among the liberated in Niger and Egypt,37 but setting prisoners free risks undermining justice systems and rule of law in the long run. It took ordinary Chadians decades to bring the brutal dictator Hissène Habré to trial in a landmark court case that set a new precedent for African justice systems.38 Sentenced to life, the 78-year-old Habré, convicted of war crimes and crimes against humanity for running a horrific regime of torture, rape, and murder that claimed some 40,000 lives, walked out of jail earlier this year, freed for fear that he might catch the coronavirus inside.39
All the while, African states must deal with ongoing conflicts. Security experts have called for a truce in the continent’s wars, but only one group in some fifteen armed conflicts across Africa has accepted40; separatists in Cameroon agreed to call off the violence for two weeks to let health workers save lives from COVID-19.41 In Libya, by contrast, fighting has actually increased during the pandemic.42 The UN Secretary-General has called for a global ceasefire during the COVID-19 crisis,43 but African terrorist organizations apparently agree with the perspective expressed by Al-Qaida core, which dubbed the virus “God’s invisible soldier” and ordered more operations against “distracted” adversaries.44 Since the start of the pandemic, terrorist groups have launched devastating attacks in Mozambique, Nigeria, Chad, Mali, and Somalia, taking a major toll on African forces.45 Terrorist violence in Burkina Faso has destroyed 100 hospitals in the country this year.46
COVID-19 is also aggravating long-term conflict drivers and undermining peaceful solutions. UN peacekeeping missions, most of which are in Africa and staffed with personnel from around the world, are struggling to carry out their mandates during the pandemic. The UN has asked nine countries to delay rotations for fear of contagion47 and the DRC has quarantined arriving UN forces rather than allowing them to deploy.48 The head of the UN mission in Mali, overseeing 15,000 peacekeepers effectively stuck in place without replacements or relief, expects the security situation to deteriorate.49 Due to coronavirus concerns, the Economic Community of West African States canceled a mission to Guinea five days before that country’s hotly contested elections; a military mutiny followed three days later.50 Weeks of rising violence and border disputes between Kenya and Somalia were meant to be eased by an Ethiopia-Kenya-Somalia head of state summit in March, but the meeting was canceled due to the coronavirus.51 The impacts of not addressing these drivers of insecurity may play out for many years to come.
Coming Out of Corona
Faced with challenges of legibility, authority, and capacity, borderline fragile states in Africa are dealing with long-standing threats while trying to rally mistrustful and recalcitrant publics, all without a clear idea of COVID-19’s progression in the population. In these circumstances, the pandemic could come to an end in Africa through different routes.
COVID-19 could be controlled through “social distancing” or eventually through a vaccine. Either case would likely reinforce divergence across Africa. More competent states would achieve containment and then test or vaccinate citizens; their successes might strengthen the social contract, if they capitalize on newfound social solidarity developed during the national emergency.52 More fragile states would demonstrate their inability to impose restrictions or to deliver an available cure to their citizens, further reducing their standing in the eyes of the population.
Alternatively, COVID-19 might race through the continent in spite of all “social distancing” efforts, overwhelming nations and infecting the vast majority of Africans. Densely populated countries and cities would be hit hardest, but contagion would continue and in time arrive in rural and remote regions. A drawn-out healthcare crisis would ensue, reaching intense levels in the coming months. Public unrest could go along with the peaks—perhaps especially, ironically, in the relatively strong states where popular expectations for government competency are higher. If they weather the storm intact, Africa’s borderline fragile states might emerge with a potential to advance. The short-term confrontations between government and population could give way, with time, to a greater sense of community through a shared experience of disaster. Ebola was stigmatized as a “disease of the poor,” but COVID-19 is already infecting Africa’s elite and powerful. Burkina Faso’s minister of foreign affairs, minister of the interior, minister of education, and minister of mines have all tested positive.53 The king of Eswatini is in critical condition struggling to breathe.54 Gates and guards cannot protect the powerful from the coronavirus; this fact could generate a new political will to ensure that hospital beds, nursing equipment, sewage systems, and drinking water are available to more than just certain categories of citizens—if nothing else, for elite self-preservation.
There are also more grim scenarios. If COVID-19 allows for reinfection, pressure on governments and societies would grow unremittingly, with very divisive results within African countries. Privileged sectors would surely desire to recover and reconnect with the outside world—if necessary, by keeping infected outcasts at bay and seeking not just “social distancing” but wholesale social separation. If COVID-19 mutates into a virus with higher mortality for lower ages, the situation could escalate quickly. The health crisis would turn into a calamity and marginal communities and desperate youths with nothing to lose could lash out against all systems, institutions, and structures. In either circumstance, African governments would eventually have to restart social life and reintegrate their nations into the global economy, despite ongoing illness and unrest inside their borders. Regression toward gatekeeper tendencies would almost certainly result from these types of changes to the current coronavirus.55
Key factors in all of these scenarios—virus mutation, reinfection rates, an eventual vaccine—depend on developments outside of Africa or beyond the control of its governments. But African states are not spectators in the coronavirus pandemic. In addition to the many specific healthcare actions already underway, African states—and especially policy-makers and officials within borderline fragile states—would do well to keep the following points in mind in their responses.

1. Navigating “Social Distancing” in Ways that Work for African People
African governments must come to terms with the reality that COVID-19 is probably spreading significantly and rapidly and that they are not positioned to fully comprehend how the infection is affecting their territories and populations. Under these conditions, punishment and coercion aimed at forcing citizens to follow “social distancing” restrictions should be only part of the response. States will need to learn the lessons from the Ebola outbreak, where people invented and shared innovative and practical solutions to deal with a deadly disease. In Guinea, Liberia, and Sierra Leone, afflicted communities championed small treatment centers, found volunteer nurses, set up community-organized quarantines, and reinvigorated local watch groups to identify potential vectors of infection.56 They also established new forms of treatment and burial that were medically safe and culturally appropriate, satisfying community expectations regarding family care for the sick and proper funerals for loved ones.
Of course COVID-19 is not Ebola, but everyday citizens are undoubtedly finding their own ways of coping with this new virus. They also have concrete policy recommendations. After 400 taxis were forced off the road in Cameroon for violating a new “three-passenger maximum” rule, the taxi union pointed out that reduced ridership ruins their business model. The union proposed to both respect the restrictions and make a living through a few reasonable options: increased fares, cuts in fuel prices, or direct subsidies.57 Such proposals deserve a hearing and a response. Governments should be listening to and collaborating with community actors to face the coronavirus.58
2. Communicating Knowledge, Concern, and Resolve Regarding Public Health and National Security
Africa’s borderline fragile states do not enjoy high levels of authority, solidarity, and social trust, but they should lose no time in building social capital. Officials should be straightforward about what is known and what is not known regarding the coronavirus, its effects in the nation, and the way the government is responding. The risk of appearing incompetent or powerless is outweighed by the urgent need to save lives and build unity. Credible voices could reinforce key messages. Governments might call on national heroes and icons—a country’s footballers or musicians—to appeal publicly to citizens to act in order to protect health workers, their communities, and themselves. Politicians should convey scientific facts rather than trafficking in promises of divine protection,59 and governments should develop tools to counter rumors, “fake news,” and propaganda.
African states also need a judicious approach regarding criminal non-state actors in the crisis. In addition to mobilizing the religious establishment for a public awareness campaign about COVID-19, the Somali government should denounce Al-Shabaab’s claims that the coronavirus is a disease brought on by “crusaders and disbelievers.” State officials should remind Somalis that the terrorist group has effectively declined a UN ceasefire offer and that it is currently showing a cynical intransigence reminiscent of its role during the 2010 to 2012 famine,60 which claimed a quarter million lives. At the same time, African governments should consider suspending, or at least softening, rebukes of criminal actors who are taking a positive role in the fight against coronavirus. Rather than criticizing them for past violence, for example, the South African police could acknowledge that the recent truce announced among Cape Town gangs will undoubtedly save lives.61 African states need effective strategic communications plans to recognize contributions against COVID-19 made by criminal elements and armed groups, without legitimizing those actors or diminishing the government’s authority.
3. Piecing Together a Post-Coronavirus Network of African Nations
As a country pulls out of its national COVID-19 emergency, it must be wise about rebuilding connections to other nations on the continent. Stronger states will need to decide when and how to open airports and borders and to restore relations with neighbors and allies. The Regional Economic Communities (RECs) are not necessarily well placed to guide and structure a re-opening. The East African Community has taken practical and forward-leaning measures,62 but most RECs have double-digit membership numbers and include at least one very weak state, which will likely slow sub-regional emergence from COVID-19 restrictions. Rather, each nation will need to make specific and pragmatic decisions. Senegal may want to support The Gambia in beating back the coronavirus, given the geographic proximity and essential interconnections between the two countries. But Dakar may also look early on to Rabat to renew their strong educational, diplomatic, and cultural ties, before reengaging completely with its immediate West African neighbors. However they are stitched together, international links among countries in Africa should be encouraged, as they will constitute a critical fabric to help lift the continent out of the pandemic.
4. Advocating for Africa’s Recovery as a Region
The African Union (AU) should orient its work toward sustainment during the crisis and advocacy for the continent’s post-coronavirus position in world affairs. The AU is an unlikely organization to coordinate or implement a full-fledged response to COVID-19 in Africa because it has limited experience in the domain of health, which until recently was something of an addendum to its agenda despite Africa’s major health challenges, including deadly diseases and pandemics. The AU’s Vision 2063, for instance, refers to a “healthy” population only vaguely and in passing,63 and none of the AU’s fourteen flagship projects—which include an integrated high-speed train network, a great African museum, and an outer space strategy—has a health focus.64 In 2017, a year when Africa counted 600 million people suffering from neglected tropical diseases (500 million of them children),65 the AU finally founded a technical institution for public health, which it created after international players intervened in the Ebola crisis. The organization is called the Africa Center for Disease Control (CDC); its Science and Programme Office is staffed exclusively by non-African senior advisors (three from the U.S. and one from China) with long experience in their own CDCs.66
Given its nascent nature and global connections, the Africa CDC might assist in getting supplies and support from organizations like the International Committee of the Red Cross, the World Health Organization, and the Carter Center (which has, through decades of investment, helped to virtually eradicate the Guinea worm throughout Africa).67 In parallel, the AU, through its main organs, should assume its role as the voice of Africa in global forums. The AU should play a part in updating standards for international air travel, facilitating the return of critical remittance flows (which have likely dwindled in the crisis),68 negotiating procedures regarding UN peacekeeper rotations, advocating for new resources to deal with refugees susceptible to infection, and so on. Without the AU’s presence, critical global decisions affecting the post-coronavirus world order could be taken without African input, with ramifications on security and governance on the continent and beyond for years to come.
For Academic Citation
Benjamin P. Nickels, “A Fragile State of Health: COVID-19 in Africa,” Marshall Center Security Insight, no. 56 (April 2020): https://www.marshallcenter.org/en/publications
/security-insights/fragile-state-health-covid-19-africa-0.
Notes
1 James C. Scott, Seeing Like a State (New Haven: Yale University Press, 1999). On legibility and its value in pandemics, see pp. 76-80. Scott’s work is a description and critique of “seeing like a state.” See also Melissa M. Lee and Nan Zhang, “Legibility and the Informational Foundations of State Capacity,” The Journal of Politics 79, no. 1 (January 2017): 118-132, accessed April 28, 2020, https://www.journals.uchicago.edu/doi/full/10.1086/688053.
2 Scott, Seeing Like a State.
3 Bronwyn Buton, “What Does the Coronavirus Mean for Africa?” AfricaSource, Atlantic Council, March 24, 2020, accessed April 22, 2020, https://atlanticcouncil.org/blogs/africasource/what-does-the-coronavirus-mean-for-africa/; see also Maxwell Bone, “Watching the Spread of Coronavirus in Côte d’Ivoire,” AfricaSource, Atlantic Council, March 31, 2020, accessed April 22, 2020, https://www.atlanticcouncil.org/blogs/africasource/watching-the-spread-of-coronavirus-in-cote-divoire/.
4 “Nombre de lits de réanimation et de respirateurs: où en est l’Afrique?” Jeune Afrique, April 8, 2020, accessed April 22, 2020, https://www.jeuneafrique.com/924087/societe/nombre-de-lits-de-reanimation-et-de-respirateurs-ou-en-est-lafrique/?utm_source=newsletter-ja-actu-abonnes&utm_medium=email&utm_campaign=newsletter-ja-actu-abonnes-09-04-20.
5 “CrisisWatch: Tracking Conflict Worldwide,” International Crisis Group, March 2020, accessed April 22, 2020, https://www.crisisgroup.org/crisiswatch/april-alerts-and-march-trends-2020.
6 Together these indicators increase the fragility score in all sub-Saharan countries except Rwanda and the island nations of Seychelles, Mauritius, and São Tomé and Príncipe. In North Africa, by contrast, these factors reduce the fragility score (in Egypt, Libya, Tunisia, Algeria, and Morocco) or have no effect on it (in Sudan).
7 These rounded figures and calculations come from numbers in two sources: “COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University,” Johns Hopkins University of Medicine Coronavirus Resource Center, accessed on April 22, 2020, “The World Factbook,” Central Intelligence Agency, accessed April 22, 2020, https://www.cia.gov/library/publications/the-world-factbook/.
8 Elzy Kolb, “75,000 People per Square Mile? These are the Most Densely Populated Cities in the World,” USA Today, July 11, 2019, accessed April 22, 2020, https://eu.usatoday.com/story/news/world/2019/07/11/the-50-most-densely-populated-cities-in-the-world/39664259/.
9 Bukola Adebayo, “Nigeria Overtakes India in Extreme Poverty Ranking,” CNN, June 26, 2018, accessed on April 22, 2020, https://edition.cnn.com/2018/06/26/africa/nigeria-overtakes-india-extreme-poverty-intl/index.html.
10 “Average Life Expectancy at Birth in 2019, by Continent and Gender (in Years),” Statista, accessed on April 22, 2020, https://www.statista.com/statistics/270861/life-expectancy-by-continent
11 Linda Nordling, “‘A Ticking Time Bomb’: Scientists Worry about Coronavirus Spread in Africa,” Science, accessed April 22, 2020, https://www.sciencemag.org/news/2020/03/ticking-time-bomb-scientists-worry-about-coronavirus-spread-africa#.
12 “CrisisWatch: Tracking Conflict Worldwide,” International Crisis Group, March 2020.
13 “Coronavirus Infects Press Freedom in Africa,” Reporters without Borders, accessed April 22, 2020, https://rsf.org/en/news/coronavirus-infects-press-freedom-africa.
14 James Gallagher, “Coronavirus: What It Does to the Body,” BBC News, accessed April 22, 2020, https://www.bbc.com/news/health-51214864.
15 See Douglass C. North, “Institutions,” The Journal of Economic Perspectives, Vol 5, No. 1 (Winter, 1991), pp. 97-112.
16 “CrisisWatch: Tracking Conflict Worldwide,” International Crisis Group, March 2020.
17 “Ibid.
18 “Ibid. See also “Guinea-Bissau: Nationwide State of Emergency in Effect as of April 3 Due to COVID-19/Update 1,” GardaWorld, April 3, 2020, accessed April 22, 2020, https://www.garda.com/crisis24/news-alerts/329081/guinea-bissau-nationwide-state-of-emergency-in-effect-as-of-april-3-due-to-covid-19-update-1; “Travel Alert: Mozambique COVID-19 Update and State of Emergency Measures (April 6, 2020),” U.S. Embassy in Mozambique, accessed April 22, 2020, https://mz.usembassy.gov/travel-alert-mozambique-covid-19-update-and-state-of-emergency-measures-april-6-2020/.
19 “How Religious Commitment Varies by Country among People of All Ages,” Pew Research Center, June 13, 2018, accessed April 22, 2020, https://www.pewforum.org/2018/06/13/how-religious-commitment-varies-by-country-among-people-of-all-ages/.
20 Amanda Lichtenstein and Rosemary Ajayi, Nwachukwu Egbunike. “Across Africa, COVID-19 Heightens Tension between Faith and Science,” March 27, 2020, From Poverty to Power, accessed on April 22, 2020, https://oxfamblogs.org/fp2p/across-africa-covid-19-heightens-tension-between-faith-and-science/.
21 “Church Coronavirus Restrictions Hit African Faithful,” France24, March 22, 2020, accessed on April 22, 2020, https://www.france24.com/en/20200322-church-coronavirus-restrictions-hit-african-faithful.
22 Moki Edwin Kindzeka, “Cameroonian Muslims Defy Coronavirus Prayer Restrictions,” VOANews, March 28, 2020, accessed on April 22, 2020, https://www.voanews.com/science-health/coronavirus-outbreak/cameroonian-muslims-defy-coronavirus-prayer-restrictions.
23 “Church Coronavirus Restrictions Hit African Faithful,” France24.
24 “CrisisWatch: Tracking Conflict Worldwide,” International Crisis Group, March 2020.
25 Ibid.
26 “Army Patrols as Moroccans Defy Virus Measures for Prayers,” Yahoo!Finance, March 22, 2020, accessed on April 22, 20202, https://finance.yahoo.com/news/army-patrols-moroccans-defy-virus-measures-prayers-144621059.html.
27 Mark Duerksen, “Innovations Needed to Prevent COVID-19 from Catching Fire in African Cities,” April 9, 2020, Africa Center for Strategic Studies, accessed on April 22, 2020, https://africacenter.org/spotlight/innovations-needed-prevent-covid-19-catching-fire-africa-cities/.
28 “Côte d’Ivoire: un centre contre le coronavirus détruit par la population à Yopougon,” Jeune Afrique, April 6, 2020, accessed on April 22, 2020, https://www.jeuneafrique.com/922182/societe/cote-divoire-un-centre-contre-le-coronavirus-detruit-par-la-population-a-yopougon/?utm_source=newsletter-ja-actu-abonnes&utm_medium=email&utm_campaign=newsletter-ja-actu-abonnes-06-04-20.
29 Jason Burke, “South African Police Fire Rubber Bullets at Shoppers amid Lockdown,” The Guardian, March 28, 2020, accessed on April 22, 2020, https://www.theguardian.com/world/2020/mar/28/south-africa-police-rubber-bullets-shoppers-covid-19-lockdown.
30 Kennedy Odede, “Kibera: Living in the Slum,” The Guardian, April 13, 2020, accessed on April 22, 2020, https://www.theguardian.com/global-development/series/kibera-living-in-the-slum. See also “Kibera Facts & Information,” Kibera UK, accessed on April 22, 20202, www.kibera.org.uk. https://www.kibera.org.uk/facts-info
31 Morris Kiruga, “Nairobi’s Fight against Coronavirus Gets Violent,” April 3, 2020, accessed on April 22, 2020, https://www.theafricareport.com/25634/nairobi-fight-against-coronavirus-gets-violent/?
32 Wendy Williams, “COVID-19 and Africa’s Displacement Crisis,” Africa Center for Strategic Studies, March 25, 2020, accessed on April 22, 2020, https://africacenter.org/spotlight/covid-19-and-africas-displacement-crisis/; “CrisisWatch: Tracking Conflict Worldwide,” International Crisis Group, March 2020.
33 Tamara Léger, “Overcrowding and the Risk of Unmitigated Spread of COVID-19 in Madagascar’s Prisons,” Amnesty International, April 3, 2020, accessed on April 22, 2020, https://www.amnesty.org/en/latest/news/2020/04/overcrowding-and-the-risk-of-unmitigated-spread-of-covid-19-in-madagascars-prisons/.
34 “CrisisWatch: Tracking Conflict Worldwide,” International Crisis Group, March 2020.
35 “Morocco to Release 5,654 Prisoners amid Coronavirus Outbreak,” MEMO Middle East Monitor, April 5, 2020, accessed on April 22, 2020, https://www.middleeastmonitor.com/20200405-morocco-to-release-5654-prisoners-amid-coronavirus-outbreak/.
36 “CrisisWatch: Tracking Conflict Worldwide,” International Crisis Group, March 2020.
37 Ibid.
38 Celeste Hicks, The Trial of Hissène Habré: How the People of Chad Brought a Tyrant to Justice (London: Zed, 2018).
39 “Chad’s Ex-Dictator Hissène Habré Granted 2 Month Release amid COVID-19 Threat,” RFI, April 7, 2020, accessed on April 22, 2020, http://www.rfi.fr/en/africa/20200407-chad-s-ex-dictator-hiss%C3%A8ne-habr%C3%A9-granted-temporary-release-amid-covid-19-threat-coronavirus-senegal.
40 Stacey Knott, “African Conflict Zones in Need of Cease-Fires for Coronavirus Aid,” VOANews, April 1, 2020, accessed April 22, 2020, https://www.voanews.com/science-health/coronavirus-outbreak/african-conflict-zones-need-cease-fires-coronavirus-aid?utm_source=Media+Review+for+April+2%2C+2020&utm_campaign=Media+Review+for+April+2%2C+2020&utm_medium=email.
41 “CrisisWatch: Tracking Conflict Worldwide,” International Crisis Group, March 2020.
42 Ibid.
43 “COVID-19: UN Chief Calls for Global Ceasefire to Focus on ‘the True Fight of Our Lives,’” UN News, March 23, 2020, accessed April 22, 2020, https://news.un.org/en/story/2020/03/1059972.
44 “TRAC Insight: Jihadists’ Propaganda Responses to Coronavirus (COVID-19),” TRAC, April 8, 2020, accessed on April 22, 2020, https://www.trackingterrorism.org/chatter/trac-insight-jihadists-propaganda-responses-coronavirus-covid-19-april-2020; Will Brown, “As the World is Distracted, Boko Haram Terrorists Strike a Key Western Ally,” Foreign Policy, April 1, 2020, accessed on April 22, 2020, https://foreignpolicy.com/2020/04/01/boko-haram-islamist-terrorists-strike-chad-while-world-distracted-by-coronavirus/.
45 Bulama Bukarti, “How Jihadi Groups in Africa Will Exploit COVID-19,” Africa in Transition, Council on Foreign Relations, April 3, 2020, accessed on April 22, 2020, https://www.cfr.org/blog/how-jihadi-groups-africa-will-exploit-covid-19; “TRAC Incident Report: Al Shabaab Suicide Bombing at Bar Bulsho Restaurant Behind Parliament Headquarters Near Security Checkpoint at Sayidka Junction in Hawlwadag District, Mogadishu, Somalia,” TRAC, March 25, 2020, accessed on April 22, 2020, https://www.trackingterrorism.org/chatter/trac-incident-report-al-shabaab-suicide-bombing-bar-bulsho-restaurant-behind-parliament-head.
46 Lisa Bryant, “Africa’s Conflict-Ridden Regions Face Another Existential Threat in COVID-19,” VOANews, April 3, 2020, accessed on April 22, 2020, https://www.voanews.com/africa/africas-conflict-ridden-regions-face-another-existential-threat-covid-19.
47 “Coronavirus: UN Asks 9 Countries to Delay Peacekeeper Rotations,” Military.com, April 8, 2020, accessed on April 22, 2020, https://www.military.com/daily-news/2020/03/08/coronavirus-un-asks-9-countries-delay-peacekeeper-rotations.html.
48 “CrisisWatch: Tracking Conflict Worldwide,” International Crisis Group, March 2020.
49 James Bays, “UN Urges Coordinated Efforts to Contain Coronavirus in Mali,” AlJazeera, April 8, 2020, accessed on April 22, 2020, https://www.aljazeera.com/news/2020/04/urges-coordinated-efforts-coronavirus-mali-200408080719265.html.
50 “CrisisWatch: Tracking Conflict Worldwide,” International Crisis Group, March 2020.
51 “Ibid.
52 Mohammed Masbah and Anna Jacobs, “Can Morocco Effectively Handle the COVID-19 Crisis?” Chatham House, April 6, 2020, accessed on April 22, 2020, https://www.chathamhouse.org/expert/comment/can-morocco-effectively-handle-covid-19-crisis-1
53 “Coronavirus Pandemic: Which Politicians and Celebs Are Affected?” AlJazeera, April 22, 2020, accessed on April 22, 2020, https://www.aljazeera.com/news/2020/03/coronavirus-pandemic-politicians-celebs-affected-200315165416470.html?xif=.
54 “Eswatini King Mswati III Criticall Ill,” NewsDay, accessed on April 22, 2020, https://www.newsday.co.zw/2020/04/eswatini-king-mswati-iii-critically-ill/.
55 Frederick Cooper, Africa Since 1940: The Past of the Present (London: Cambridge University Press, 2002).
56 Paul Richards, “What Might Africa Teach the World ? COVID-19 and Ebola Virus Disease Compared,” African Arguments, accessed on April 22, 2020, https://africanarguments.org/2020/03/17/what-might-africa-teach-the-world-covid-19-and-ebola-virus-disease-compared/.
57 Moki Edwin Kindzeka, “In Cameroon, Violating COVID-19 Restrictions Can Get You Arrested,” VOANews, accessed on April 22, 2020, https://www.voanews.com/science-health/coronavirus-outbreak/cameroon-violating-covid-19-restrictions-can-get-you-arrested.
58 W. Gyude Moore, “Curfews Are a Safer Plan Than Total Lockdowns to Slow COVID-19’s Spread in Informal Economies,” QuartzAfrica, accessed on April 22, 2020, https://qz.com/africa/1836458/curfews-not-lockdowns-will-slow-covid-19-spread-in-africa/.
59 “Burundi Shrugs Off Pandemic, Citing ‘God’s Protection,’” Daily Nation, April 10, 2020, accessed on April 22, 2020, https://www.nation.co.ke/news/africa/Covid-19-pandemic--Burundi-cites--God-s-protection-/1066-5519714-iaaqm/index.html.
60 “Coronavirus: Fighting Al-Shabab Propaganda in Somalia,” BBC News, April 2, 2020, accessed on April 22, 2020, https://www.bbc.com/news/world-africa-52103799.
61 “How Coronavirus Inspired a Gangland Truce in South Africa,” BBC News, April 8, 2020, accessed on April 22, 2020, https://www.bbc.com/news/av/world-africa-52205158/how-coronavirus-inspired-a-gangland-truce-in-south-africa.
62 “Coronavirus Disease (COVID-19) Outbreak,” East African Community, accessed on April 22, 2020, https://www.eac.int/coronavirus.
63 “Agenda 2063: The Africa We Want,” The African Union, accessed on April 22, 2020, https://au.int/en/agenda2063/overview.
64 “Flagship Projects of Agenda 2063,” The African Union, accessed on April 22, 2020, https://au.int/agenda2063/flagship-projects.
65 Matshidiso Rebecca Moeti, “Accelerating the Control and Elimination of Neglected Tropical Diseases in Africa,” SpeakUpAfrica, April 28, 2017, accessed on April 22, 2020, https://www.speakupafrica.org/2017-4-28-accelerating-the-control-and-elimination-of-neglected-tropical-diseases-in-africa/.
66 “Staff Directory,” Africa CDC, accessed on April 22, 2020, https://africacdc.org/staff-directory/.
67 “Guinea Worm Eradication Program,” The Carter Center, accessed on April 22, 2020, https://www.cartercenter.org/health/guinea_worm/.
68 Fatima Lahnait, “L’impact du COVID-19 sur les transferts d’argent de la diaspora: la solidarité au-delà des frontières,” Timbuktu Institute, African Center for Peace Studies, April 10, 2020, accessed on April 22, 2020, https://timbuktu-institute.org/index.php/toutes-l-actualites/item/324-l-impact-du-covid19-sur-les-transferts-d-argent-de-la-diaspora-la-solidarite-au-dela-des-frontieres
About the Author
Benjamin P. Nickels is professor of international security studies at the Marshall Center, where he also serves as course director of the Europe-Africa Security Seminar. Prior to joining the Marshall Center in 2018, Dr. Nickels was academic chair for transnational threats and counterterrorism at the Africa Center for Strategic Studies. Dr. Nickels’ research focuses on political violence, displaced populations and migration, counterterrorism and counterinsurgency, and security cooperation in Europe, Africa, and the Middle East. He has received numerous awards, including a Fulbright scholarship to Morocco and a Chateaubriand fellowship in France. He holds a doctorate with distinction in history from the University of Chicago.
The Marshall Center Security Insights
The George C. Marshall European Center for Security Studies in Garmisch-Partenkirchen, Germany, a German-American partnership, is committed to creating and enhancing worldwide networks to address global and regional security challenges. The Marshall Center offers fifteen resident programs designed to promote peaceful, whole of government approaches to address today’s most pressing security challenges. Since its creation in 1992, the Marshall Center’s alumni network has grown to include over 14,000 professionals from 156 countries. More information on the Marshall Center can be found online at www.marshallcenter.org.
The articles in the Security Insights series reflect the views of the authors and are not necessarily the official policy of the United States, Germany, or any other governments.


